



Request Call Back
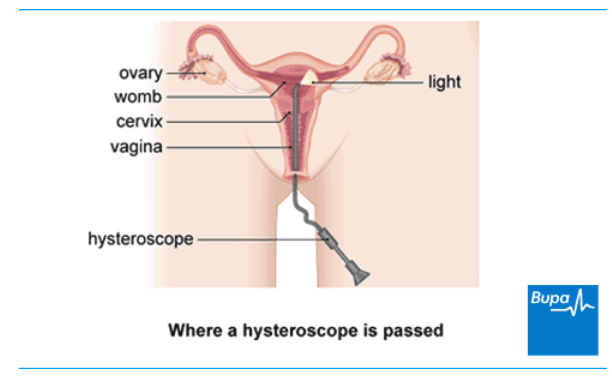
A hysteroscopy is a procedure to look inside your womb (uterus) to check for any problems. Sometimes, a problem can be treated at the same time. A hysteroscopy is done with a narrow tube-like telescope with a camera. This is called a hysteroscope. A specialist doctor (gynaecologist) will put the hysteroscope into your vagina and then pass it up through the neck of your womb (cervix) and into your womb.
You may have a hysteroscopy for the following reasons.
Your hospital will tell you how to prepare for your hysteroscopy procedure. If you’re still having periods, you need to be sure there’s no chance that you’re pregnant at the time of your procedure. For this reason, it’s important to use contraception or not have sex between your last period and the test.
Don’t worry if you’re bleeding at the time of your procedure. Your hysteroscopy can usually go ahead, unless it’s heavy, but check with your hospital.
You’ll usually have the procedure and go home on the same day.
Your hospital might tell you to take an over-the-counter painkiller such as ibuprofen (a non-steroidal anti-inflammatory medicine) an hour or two before your procedure.
You may not need an anaesthetic or you may have a local anaesthetic. You may be able to have a general anaesthetic if you prefer or if you’re having a longer and more complicated operation such as having fibroids treated. This means you’ll be asleep during the operation. A general anaesthetic can make you sick so it's important that you don't eat or drink anything for six hours before your hysteroscopy. Follow your anaesthetist or doctor or specialist nurse’s advice and if you have any questions, just ask.
Your nurse or doctor will discuss with you what will happen before, during and after your procedure, including any pain you might have. If you’re unsure about anything, ask. No question is too small. It’s important that you feel fully informed so you’re in a position to give your consent for the operation to go ahead. You’ll be asked to sign a consent form.
A hysteroscopy usually takes about 10 to 15 minutes but it depends on what you are having it for. Your doctor or specialist nurse will ask you to lie down with your legs up. You can put your legs into supports.
There are two main ways your doctor may do a hysteroscopy.
With both techniques, your doctor or specialist nurse will then put a sterile (clean) fluid into your womb to make it bigger, which helps your doctor or specialist nurse to see clearly. The camera on the hysteroscope sends pictures of the inside of your womb to a monitor where your doctor or specialist nurse can see it. They’ll look at these images and take a sample of tissue (biopsy) or do any treatment that’s needed. You can usually see this on the monitor too.
A hysteroscopy can be uncomfortable and sometimes painful, and you might have some pain like period pains while the hysteroscopy is being done. If you find it too painful, tell your doctor and they’ll stop.
If you didn’t have an anaesthetic or had a local anaesthetic, you should be able to go home a short time after your procedure.
If you had a general anaesthetic, you’ll need to rest until the effects have passed and then, when you feel ready, you can go home. Make sure someone can take you home. And ask someone to stay with you for a day or so while the anaesthetic wears off. Having a general anaesthetic can really take it out of you. You might find that you're not so coordinated or that it's difficult to think clearly. This should pass within 24 hours. In the meantime, don't drive, drink alcohol, operate machinery or sign anything important.
You might have some discomfort as the anaesthetic or painkiller wears off. You can take over-the-counter painkillers, such as paracetamol or ibuprofen if you need to.
You may have some bleeding from your vagina. You can use sanitary pads until the bleeding stops – it’s best not to use tampons.
Your nurse may give you a date for a follow-up appointment. If your doctor took tissue samples, it can take a couple of weeks to get the results.
Most women don’t have any problems after having a hysteroscopy. But contact your doctor or go to the accident and emergency department of your local hospital if you have:
If you had your hysteroscopy as an out-patient with no anaesthetic, you should be able to go back to your usual activities the same day. But take a day or two off work to recover if you can. If you’ve had a general anaesthetic and treatment, it’s likely to take longer to get back to normal so get plenty of rest for a few days.
It’s normal to have some period-like cramping pains and some bleeding for a few days after your hysteroscopy. If you need pain relief, you can take over-the-counter painkillers.
You can usually exercise when any bleeding and pain has settled down. It’s best to wait a week until you have sex. And most importantly, wait until you feel ready.
Side-effects are the unwanted but mostly temporary effects that you may get after having the procedure.
After a hysteroscopy, you may have:
Complications are when problems occur during or after your procedure. The possible complications of a hysteroscopy include the following.
The risk of complications is higher if you have a hysteroscopy under general anaesthesia.
Depending on what’s causing your symptoms, you may need to have other tests as well as or instead of a hysteroscopy. These include the following.
Your doctor will talk to you about the treatment or investigation options for you.
Dilation and curettage (D&C) is a surgical procedure. A doctor opens your cervix (dilation) and uses an instrument to remove some of the lining of your womb (curettage). This can help to diagnose and treat a condition that may be causing any abnormal bleeding. You might also have a D&C after a miscarriage, to remove any tissue that’s left behind in your womb. Hysteroscopy is where your doctor or specialist nurse uses a camera to look at the inside of your womb. They may then use instruments to take a sample of tissue or treat a gynaecological condition. You would usually have a hysteroscopy first to look at your womb, then have a D&C afterwards this if necessary.
D&C is used less and less, since newer techniques have replaced it.
Unusual vaginal bleeding is relatively common, and around one in every four women will have it at some point in life. Some kinds of unusual bleeding are linked to your periods, but others aren’t. Here are some of the main types of unusual bleeding.
There are several conditions that can cause unusual vaginal bleeding, but sometimes your doctor won’t be able to find a specific cause. If you have unusual vaginal bleeding, go and see your doctor.