



Request Call Back
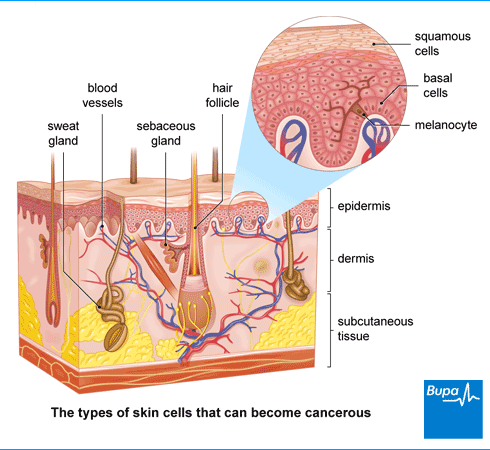
The two main types of non-melanoma skin cancer form in cells in the top layer of your skin (the epidermis). They are described below.
Basal cell carcinoma (BCC) is a type of cancer that starts in the basal cells which form the bottom layer of your epidermis. It’s the most common form of skin cancer.
BCCs grow slowly and don’t usually spread to other parts of your body, but they can grow into the healthy tissues surrounding the site of the cancer. These types of cancer are most common in middle-aged and elderly people, although they are becoming more common in younger people.
Squamous cell carcinoma (SCC) is a type of cancer that starts in the flattened (squamous) cells which form the top layer of your epidermis.
Squamous cell carcinomas (SCCs) usually grow more quickly than basal cell carcinomas (BCCs) and may spread into other parts of your body. You’re also more likely to get an SCC as you get older .
The symptoms of skin cancer vary a lot between people. If you have skin cancer, you’re likely to notice an abnormal change to an area of your skin. This might be a new lump on your skin, a scaly, itchy or crusty raised area of skin or a scab that doesn’t heal. Basal cell carcinomas and squamous cell carcinomas have some differences in how they may look.
Basal cell carcinomas may look like:
With either type of non-melanoma skin cancer, you may notice the lump or area of skin ulcerates (breaks the skin) and crusts or bleeds. This may heal, and then ulcerate again repeatedly.
A new mole or change in an existing mole (for example, a change in size, shape or colour) can be the first sign of melanoma. This is a more serious type of skin cancer.
It’s important to get any unusual change to your skin checked out with a doctor, particularly if it’s not healing or getting worse over time.
Your doctor will ask you about your symptoms and examine you. They may ask you questions about your medical history, and about how much exposure you’ve had to the sun or sunbeds in the past.
Your doctor may suspect you have a non-melanoma skin cancer just from how it looks. But you’ll need to have a biopsy to confirm the diagnosis. This is where a sample of tissue is taken and sent to a laboratory to be tested for cancer cells.
A biopsy can often involve removing the whole area of skin that your doctor thinks may be cancerous, along with some healthy skin (an excision biopsy). For many people, this may be all that’s needed – so diagnosis and treatment can be done at the same time. Sometimes, your doctor may remove just a sample of the affected skin. You’ll then need further treatment once your diagnosis is confirmed.
If you have a basal cell carcinoma (BCC), your doctor may be able to do the excision biopsy themself. In certain circumstances – for instance, if your BCC is large or in an awkward place – they may refer you to a dermatologist or plastic surgeon. A dermatologist is a doctor who specialises in skin conditions. You’ll also be referred to a specialist if your doctor suspects you have a squamous cell carcinoma.
You won’t usually need any further tests if you’ve been diagnosed with a non-melanoma skin cancer. But if you have a particularly aggressive type of cancer, your doctor may recommend tests to check if it has spread.
Most of the time, non-melanoma skin cancers can be treated with minor surgery. But there are alternatives to surgery that may be more suitable for some people.
The treatment you have will depend on:
Your doctor will discuss your treatment options with you.
An excision is a procedure to remove the cancer, along with some of the surrounding healthy skin to make sure it’s completely removed. This is the most common treatment both for basal skin carcinoma and squamous cell carcinoma, and often it’s the only treatment that’s needed. A small wound can be closed with stitches, but if you have a large area of skin removed, you may need a skin graft. See our FAQs below for more information about skin grafts and skin flaps.
This is a more specialised type of surgery. You may have it for a basal cell carcinoma or squamous cell carcinoma in an area that’s difficult to treat, such as your head or neck. You may also have Mohs surgery if your cancer has come back. In Mohs surgery, your surgeon will remove layers of the affected skin in stages. They’ll look at the removed layer under a microscope straight away to check if all the cancer has been removed. This is repeated until all the cancer has been taken away.
This treatment is sometimes offered if you have basal cell carcinoma or a low-risk squamous cell carcinoma. It involves This treatment is sometimes offered if you have basal cell carcinoma or a low-risk squamous cell carcinoma. It involves cutting away the affected part of your skin, then using an electric needle to destroy any cancer cells left behind. The technique is usually repeated three times during one appointment.
Non-surgical treatments can be an option for some people with low-risk non-melanoma skin cancer – mainly basal cell carcinomas.
Non-surgical treatments include the following.
You may be offered radiotherapy and/or chemotherapy alongside other treatments if you have a squamous cell carcinoma that has spread to other parts of your body.
Over-exposure to ultraviolet (UV) radiation from the sun or sunbeds is one of the main causes of all types of skin cancer.
In non-melanoma skin cancer, having a lot of exposure to the sun over time puts you at greater risk of developing a cancer. In contrast, having intermittent, intense periods of exposure, especially in childhood, is a greater risk factor for melanoma.
You’re at greater risk of non-melanoma skin cancer if you:
You may also be at greater risk of squamous cell carcinoma (SCC) in particular if you have a weakened immune system. This could be because you take medicines that suppress your immune system or you have a disease that affects your immune system.
Sometimes, SCC can develop if you have had skin damaged in other ways. For instance, damage from other forms of radiation, burns or persistent ulcers and wounds in the skin.
The following tips may help to protect your skin from burning and reduce your risk of developing skin cancer.
If you have patches of sun-damaged skin, known as an actinic keratosis, it’s important to get this treated to reduce the chance of it turning into a squamous cell carcinoma.
When you have skin cancer surgically removed, some of your healthy skin may have to be removed too. If this is a large area and can’t heal on its own or with stitches, you may need to have the skin replaced. This is usually done with a skin graft or skin flap.
A skin graft is a thin layer of skin taken from another area of your body and placed over the area where the cancer was removed. A graft is usually held in place with stitches and a dressing will be placed over it.
The area that the healthy skin was taken from will either be closed with stitches or left to heal by itself under a special dressing. It may feel sore, and can take up to two weeks to heal, depending on where the skin was taken from. After it’s healed, the skin may look different from your surrounding skin and may be a slightly different colour.
A skin flap is a thicker layer of skin than a graft. It’s taken from an area close to where your cancer has been removed. The blood supply to the skin flap is left intact – this will help it to heal. The flap is held in place with stitches and a dressing will be placed over it. Skin flaps may give a better cosmetic result (look better). This is because they use skin that is similar to the colour, type and thickness of the skin that has been removed.
Your surgeon will discuss which option is best for you and will explain what is involved in these procedures.
The most serious type of skin cancer is melanoma. Non-melanoma skin cancers can usually be cured and are very rarely life-threatening.
Basal cell carcinomas (BCCs) can almost always be cured. They can be more difficult to treat if they’ve been left for a long time or if they’re in an awkward place. They can also sometimes come back after treatment (called a recurrence). But it’s extremely rare for BCCs to spread (metastasise).
Most squamous cell carcinomas (SCCs) are also low-risk and can usually be cured. However, a very small number of SCCs can spread to other parts of the body. These cancers can be life-threatening. Because they can potentially be more dangerous, you’ll get an urgent referral to a specialist if your doctor suspects you may have an SCC.
www.cancerresearchuk.org
www.macmillan.org.uk
www.skinhealthinfo.org.uk