



Request Call Back
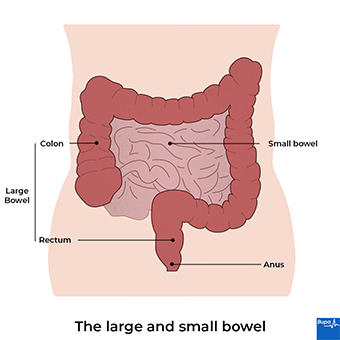
There are lots of types of bowel surgery. This information is about surgery to remove all or part of your large bowel (colon). This is called a bowel resection. You might need this type of surgery if you have a bowel condition such as bowel cancer, diverticular disease, Crohn’s disease or ulcerative colitis.
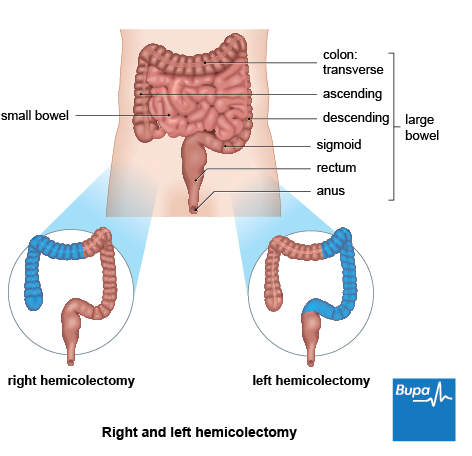
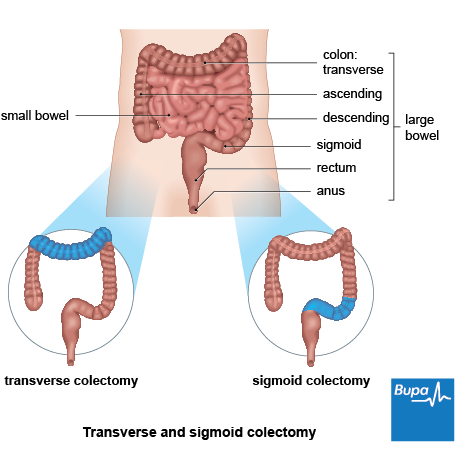
The exact procedure you have will depend on the reason why you’re having surgery and how much of your bowel is affected. The procedures are named differently depending on what section of bowel is removed. They include:
Some of these types are shown in the illustrations below. Your surgeon will talk with you about the most appropriate procedure for you.
If your doctor recommends surgery, they’ll go through exactly what to expect with you. This will include what will happen before, during and after your procedure, and the risks and benefits involved. Do ask your doctor if you have any questions or need any more explanation about the procedure. You’ll be asked to sign a consent form before the procedure, so it’s important that you feel fully informed.
You’ll be assessed before your operation to check that you’re fit for surgery. This will often happen at a preoperative assessment clinic. They’ll also explain how to prepare for your operation. For example, if you smoke, you’ll be asked to stop because smoking increases your risk of infections and other complications after surgery. The nurse or doctor will check what medicines you’re taking and advise if you should stop taking any of them before surgery.
Sometimes, you may be asked to take laxatives on the day of your surgery or the night before, to clear out your bowel. Or you may need to have an enema – a small amount of liquid medicine is inserted into your back passage (rectum) to help you to empty your bowel.
Bowel resection usually involves a hospital stay of between three and nine days, so it’s important that you make any necessary preparations for this.
You’ll have bowel resection surgery under general anaesthesia[PC1] , which means you’ll be asleep during your operation. You’ll be given clear instructions about when to stop eating and drinking before your anaesthetic. You may be given a special, carbohydrate-rich drink to have the night before your surgery and again a few hours beforehand.
When you come into hospital, a member of the surgical team will talk you through what will happen and answer any questions you may have. They’ll check that you’re well and still happy to go ahead. You may be asked to wear compression stockings and you may be given an injection of an anti-clotting medicine called heparin. This helps to prevent blood clots forming in the veins in your legs. You may also have an antibiotic injection before your operation to reduce your risk of infection.
Bowel resection surgery involves removing the diseased parts of your bowel and, if possible, joining the two healthy ends together using stitches or staples. This is called an anastomosis.
Sometimes, your surgeon may need to bring the healthy end of your bowel through your abdominal wall and onto the surface of your skin. This is called a stoma. If the operation involves your large bowel, it’s called a colostomy; if it involves your small bowel, it’s called an ileostomy. The waste from your bowel passes out of the stoma, and is collected in a bag that you wear over the stoma. A stoma can either be temporary or permanent, depending on the type of surgery you have and how much bowel your surgeon removes.
If your surgeon thinks you may need a stoma, they’ll arrange for you to see a specialist stoma nurse before your operation. Our FAQs explain in more detail how a colostomy may affect your everyday life.
If you’re having a proctocolectomy to remove all your large bowel and back passage, your surgeon may create a ‘pouch’ from the end of your small bowel. This can store the waste from your bowel and allow you to pass waste (poo) through your anus.
There are two main ways you can have bowel surgery: keyhole (laparoscopic) and open surgery.
People often recover more quickly from keyhole surgery, don’t have to stay in hospital for so long and may have less pain afterwards. Not everyone can have keyhole surgery though – it depends on your circumstances. Sometimes your surgeon will need to switch from keyhole to open surgery during the operation. They’ll talk to you about the possibility of this happening, and what it will mean, before your surgery.
A newer type of surgery that uses robotics is being used in some hospitals for surgery on the back passage (rectum). This is a new technique that’s still under investigation, so it’s not available everywhere yet.
You’ll spend the first few hours after your operation in a special recovery unit, before being transferred to a ward or other unit. You might have some discomfort as the anaesthetic wears off, but you’ll be offered pain relief as you need it. The two most common types of pain relief you may have are patient-controlled analgesia and an epidural. In patient-controlled analgesia, morphine is delivered directly into a cannula or drip. In an epidural, a pain-relieving medicine is injected into the space that surrounds your spinal cord (the epidural space).
At first, you’ll have a catheter to drain urine from your bladder into a bag. You may also have fine tubes (drains) running out from your tummy to drain fluid into another bag. These are usually removed after a few days. You’ll have a drip in your hand or arm to give you fluids. This can usually be removed after a day or so. You’ll be encouraged to eat and drink as soon as you feel ready. Read our FAQ on what to eat after bowel surgery for more information.
To help prevent deep vein thrombosis (DVT), you’ll have a daily injection of an anti-clotting medicine and be asked to keep wearing compression stockings. You’ll also be encouraged to get out of bed and move around as soon as possible. You may be shown exercises you can do while sitting or lying down too, including breathing exercises to clear your lungs.
You’ll be able to go home a few days after surgery but exactly when will be different for everyone. It’ll depend on the type of surgery you had and how well you’re recovering. Before you go home, your nurse will give you some advice on how to care for your healing wounds and stoma if you have one. If you have a stoma, you’ll be given the details of a stoma nurse you can contact once you get home, if you need to.
It usually takes at least six weeks to start feeling that you’re back to normal after bowel surgery. You should avoid heavy lifting and strenuous exercise for longer than this though.
You might continue to have some pain and discomfort from your surgery for a while. You may be prescribed some painkillers to take home, but you can also take over-the-counter painkillers, such as paracetamol or ibuprofen if you need to. Always read the patient information that comes with your medicine and if you have any questions, ask your pharmacist for advice.
It can take a while for your bowel to settle down after surgery. Your doctor may suggest some changes to your diet while your bowel is recovering. For more information, read our FAQ on what to eat after bowel surgery.
It’s common to feel tired while you’re recovering and to need to sleep and rest more than usual. It’s important to take time to rest. But do try to get up and move around as much as you can, and keep up any exercises you’ve been given by your physiotherapist. This can help you to feel better and get your strength back as well as reduce your risk of complications.
Complications are problems that can happen during or after your surgery. The possible complications of any operation include an unexpected reaction to the anaesthetic or developing a chest infection afterwards. Complications may also include excessive bleeding or developing a blood clot, usually in a vein in your leg (deep vein thrombosis, DVT).
Specific complications of bowel surgery include the following.
You’ll often be advised to follow a low-fibre diet while you recover from surgery. This means choosing foods such as white bread, pasta and plain crackers, and only eating fruit and vegetables that have been well-cooked or peeled. It’s common to get diarrhoea after bowel surgery, and this can help to prevent it.
Bloating and excess wind are common after bowel surgery, so it’s a good idea to avoid foods and drinks that may cause this. These include onions, garlic, beans, fizzy drinks, lager and beer. Peppermint and fennel tea might help to relieve these symptoms.
Try to eat smaller, more frequent meals that are high in calories and protein such as meat, fish and eggs, to help your body heal. Make sure you chew your food slowly and thoroughly, to avoid getting wind.
As your bowel heals and settles down, you may be able to reintroduce certain foods. It may help to keep a food diary, so you can track how different foods affect you. If your bowel movements don’t seem to be returning to normal, ask your doctor or dietitian for advice.
Having surgery near your back passage (rectum) may affect your pelvic nerves, leading to difficulties when you have sex. Men might experience erection or ejaculation problems, while women may have reduced sensitivity and changes to their vagina, which might make sex painful. Do talk to your doctor if this is affecting you, as they may be able to prescribe medicines to help. Sometimes these problems improve over time.
If you have large scars or a colostomy (or ileostomy) bag because of a stoma, you may feel self-conscious about having sex. You should discuss these concerns with your specialist stoma nurse who will be able to help and provide advice and support.
Having a colostomy or ileostomy bag shouldn’t stop you doing any of the things you used to do. But it can take time to get used to having one and you may need to make slight adjustments and plan ahead more.
Before you leave hospital, a specialist stoma nurse will show you how to care for your stoma and your colostomy or ileostomy bag. The bags are designed to fit discreetly under normal clothing. They shouldn’t leak or smell (except while being changed, and you can buy products to reduce any odour). You can bath or shower with one on.
Your stoma nurse may visit you at home to give you more advice on day-to-day activities. For instance, you can get a device to stop your seat belt pressing on your stoma and the bag while driving. There’s no reason why you shouldn’t return to work, but in some circumstances, you may need to make some adjustments. For instance, if your work involves heavy lifting or other tasks that puts a strain on your abdominal muscles, you may need to wear a support garment or consider changing your duties to less strenuous tasks.
You won’t usually need a special diet if you have a stoma. But you might need to make some changes to your diet while you recover from surgery. For more information, see our FAQ on what foods to eat. Some foods may make you uncomfortable – it’s worth keeping a food diary to keep track of what affects you.
Lots of people and places can support you in adapting to having a stoma. Our section on other helpful websites gives details of several helpful and supportive organisations.